26 June 2026
Table of Contents
A glioblastoma diagnosis is one of the most confronting things a patient or family can face. It is the most aggressive primary brain tumour, and the honest truth is that it is a serious, difficult disease. At the same time, the decisions made in those first weeks, about where to be treated, which team to trust and what the treatment plan looks like genuinely matter. This guide is here to help you make those decisions well.
Glioblastoma treatment in India has advanced significantly. Experienced neuro-oncology teams, modern surgical technology, advanced radiation techniques, and growing access to clinical trials mean that patients in India today have access to world-class care without needing to travel abroad. The question is not whether good treatment exists because it does. The question is how to find it, evaluate it, and choose the approach that gives you the best possible outcome for your specific tumour and circumstances.
What Is Glioblastoma and Why Is It So Challenging?
Glioblastoma multiforme (GBM) now classified as Glioblastoma, IDH-wildtype, Grade 4 is the most common and most aggressive primary brain tumour in adults. It arises from glial cells which are the supportive cells of the brain and is characterised by rapid growth, extensive invasion of surrounding brain tissue and a strong tendency to recur after treatment.
What makes glioblastoma particularly challenging is its biology. Unlike many other tumours that grow in a contained mass, glioblastoma sends microscopic tendrils into the surrounding brain tissue, making complete surgical removal impossible. These infiltrating cells survive treatment and drive recurrence. The blood-brain barrier also limits which drugs can reach the tumour effectively, narrowing the systemic treatment options compared to other cancers.
Glioblastoma is diagnosed in around 3-4 per 100,000 people per year, making it relatively rare but disproportionately serious. It can occur at any age but is most commonly diagnosed in adults between 45 and 70. Median survival with standard treatment has historically been around 14-16 months, though this varies considerably based on molecular factors, surgical outcome, and performance status and a meaningful proportion of patients live significantly longer.
Why Molecular Testing Is Non-Negotiable
Before discussing treatment choices, there is one thing that needs to happen first and it is the single most important step after diagnosis that families often don’t know to ask about: comprehensive molecular testing of the tumour tissue.
Not all glioblastomas behave the same way. The molecular characteristics of the tumour, specific genetic markers profoundly influence how it responds to treatment and what additional options may be available. The three most critical markers to test for are:
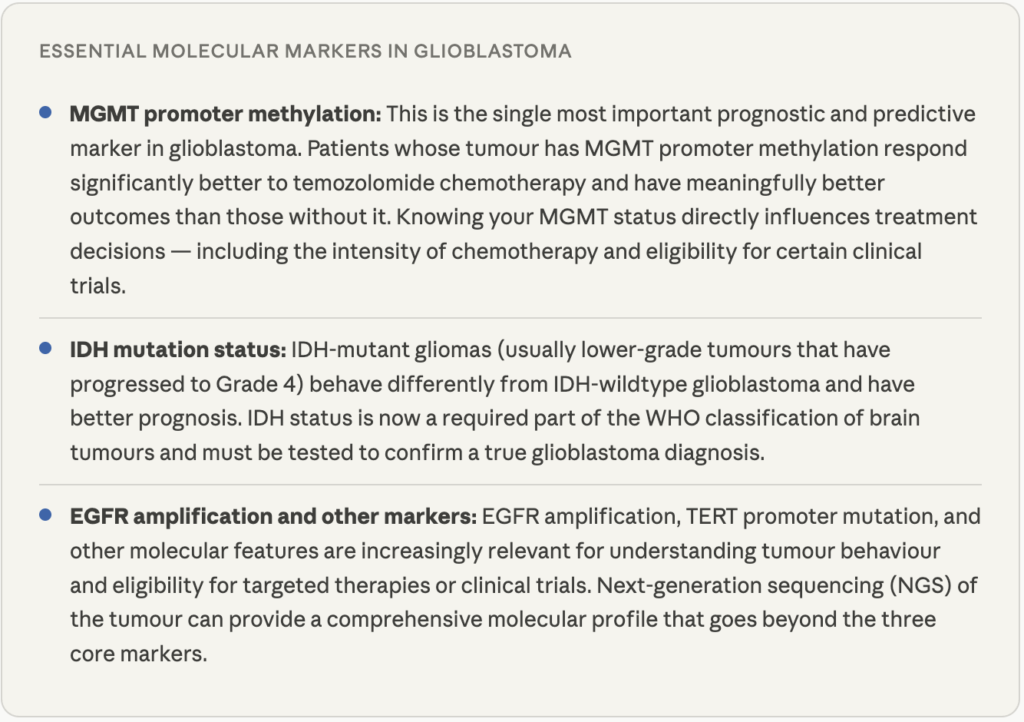
If the team managing your case has not discussed molecular testing or if the pathology report doesn’t include MGMT and IDH status, ask explicitly. This is non-negotiable standard of care for glioblastoma in 2024 and beyond. Any specialist centre worth choosing will offer this routinely.
Key Factors to Consider When Choosing Glioblastoma Treatment in India
This is the heart of what this guide is here to help with. When evaluating treatment
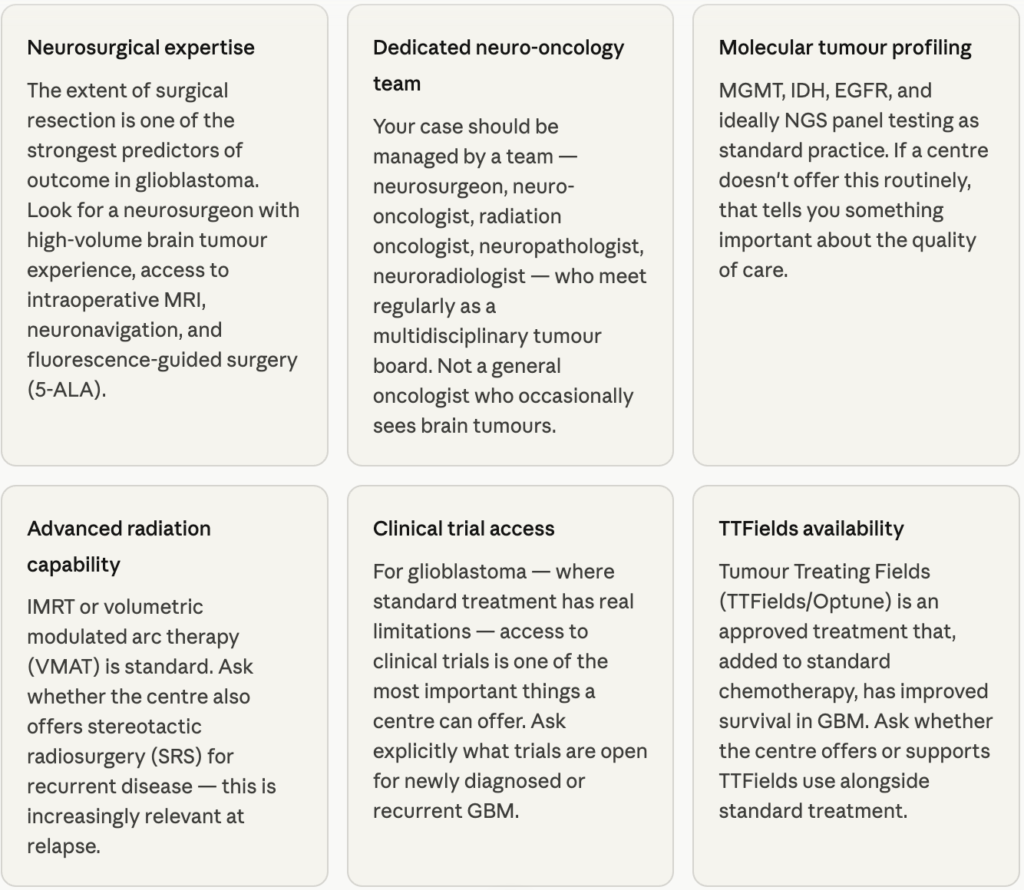
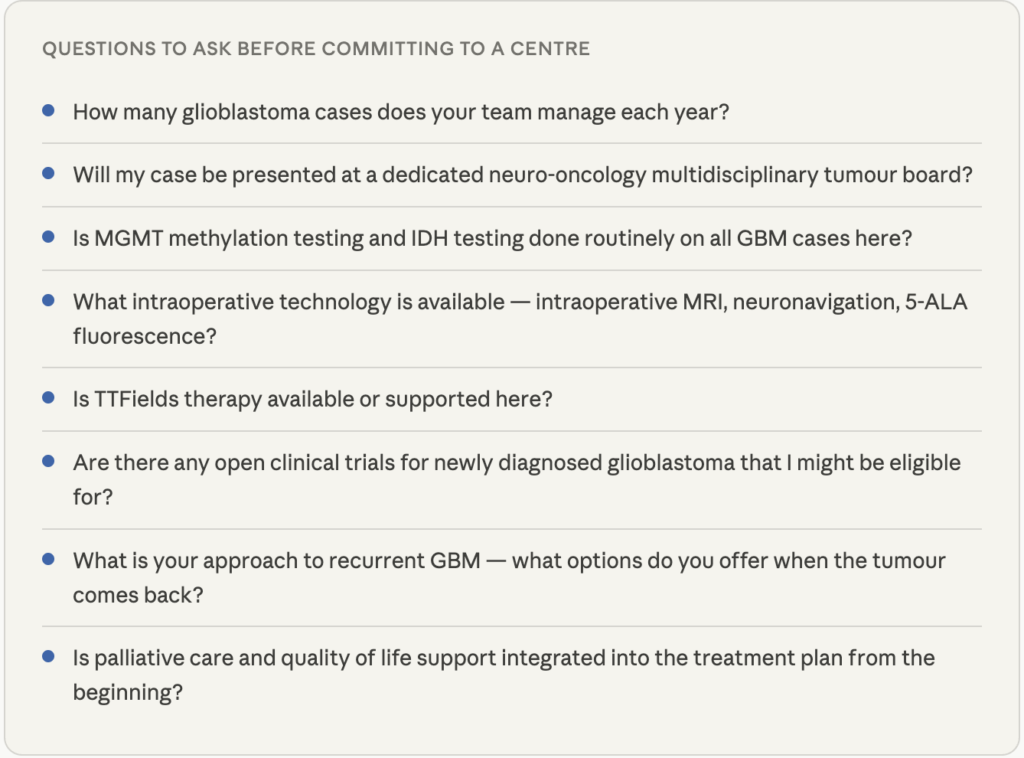
A centre that answers these questions openly, confidently, and without defensiveness is one that takes glioblastoma seriously.
What Does Standard Glioblastoma Treatment Involve?
Standard of care for newly diagnosed glioblastoma has been established for nearly two decades, the Stupp protocol and involves three phases used in sequence:
Surgery - maximal safe resection
The goal of surgery is to remove as much of the tumour as safely possible while preserving neurological function. This is called maximal safe resection. Studies consistently show that a greater extent of resection is associated with longer survival, which is why the surgeon’s skill and the technology available in the operating theatre matter so much.
Modern neuro-oncology centres use intraoperative MRI to confirm the extent of resection in real time, neuronavigation to precisely locate the tumour in three dimensions and 5-ALA fluorescence-guided surgery, where a dye taken before the operation causes tumour cells to glow pink under a specific light, helping the surgeon distinguish tumour from healthy brain tissue. In some cases, awake craniotomy where the patient is awake during part of the surgery, is used to preserve speech and motor function while maximising tumour removal.
Complete resection is rarely achievable given glioblastoma’s infiltrative nature, but the amount of tumour removed at surgery is one of the most modifiable determinants of outcome making surgical expertise the first thing to evaluate when choosing where to be treated.
Concurrent chemoradiation - the Stupp protocol
After surgery, the standard treatment is six weeks of daily radiation to the tumour bed combined with daily temozolomide chemotherapy. This concurrent chemoradiation phase is followed by six months of maintenance temozolomide. The benefit of adding temozolomide to radiation is greatest in patients whose tumour has MGMT promoter methylation, which is another reason this testing is so important before starting treatment.
TTFields (Tumour Treating Fields) an approved wearable device that delivers low-intensity electric fields to disrupt tumour cell division can be added alongside maintenance chemotherapy. It has been shown to extend survival when used consistently and is increasingly available in India.
Supportive care throughout
Steroids (typically dexamethasone) are used to manage brain swelling and associated symptoms. Anti-seizure medications may be prescribed. Rehabilitation, physiotherapy, speech therapy, cognitive support, is an important part of maintaining quality of life through treatment. These are not afterthoughts, they are integral to managing glioblastoma well.
When Glioblastoma Recurs: Treatment Options in India
Glioblastoma almost always recurs, typically within 6-9 months of completing initial treatment. This recurrence is anticipated, and a good neuro-oncology team begins thinking about it from the outset. When recurrence happens, the approach depends on several factors: where the tumour has recurred, the patient’s current neurological condition and performance status, what treatment has already been given, and what options are available.
Repeat surgery
For accessible recurrences in patients who are in good enough condition, repeat surgery can extend survival and relieve symptoms. The decision is nuanced, the benefit of re-operation depends significantly on how much tumour can be removed and what the impact on neurological function would be. An experienced neuro-oncology team will assess this honestly rather than defaulting to surgery in every case.
Re-irradiation
Stereotactic radiosurgery (SRS) or hypofractionated re-irradiation can be used to treat localised recurrences. This is increasingly available at advanced radiation oncology centres in India. The feasibility depends on how much radiation was given initially and what area of the brain is affected.
Systemic treatment at recurrence
Bevacizumab, an anti-VEGF agent that targets the tumour’s blood supply is commonly used at recurrence in glioblastoma, either alone or in combination with chemotherapy. Lomustine (CCNU) and other second-line chemotherapy agents are also used. Response rates are modest, but these treatments can provide a period of disease control and symptom improvement.
Clinical trials at recurrence
This is perhaps the most important point for families facing recurrent glioblastoma. Clinical trials at recurrence represent the most meaningful avenue for accessing newer therapies, immunotherapy approaches, targeted agents, novel delivery systems that are not yet standard but are showing promise. India has growing participation in international neuro-oncology trials. Ask your team explicitly what trials are open for recurrent GBM when the time comes.
Quality of Life - A Core Part of the Treatment Conversation
With glioblastoma, quality of life is not a secondary concern, it is central to every treatment decision. Because the tumour affects the brain, treatment decisions have direct implications for how a person thinks, speaks, moves, and experiences daily life. A good neuro-oncology team keeps this at the centre of every conversation.
Early integration of palliative care, specialist support for symptom management and quality of life is strongly recommended in glioblastoma, not as a signal that treatment is ending, but because it genuinely improves treatment adherence and patient wellbeing when introduced from the start. Patients who receive early palliative care alongside active treatment consistently do better on quality of life measures and often maintain treatment for longer.
Cognitive rehabilitation, physiotherapy, speech and language therapy, and psychological support for both the patient and family are all important parts of comprehensive glioblastoma care. Ask your centre what is available and whether these services are embedded in the care pathway or referred out separately.
There is also the conversation about goals of treatment, what matters most to you, how you want to spend your time, what quality of life means for your specific situation. A neuro-oncology team that creates space for these conversations, rather than defaulting purely to maximum treatment at all costs, is one that treats the whole person. That is something worth looking for.
Frequently Asked Questions
Glioblastoma is treated in India, and experienced neuro-oncology teams with access to modern surgical technology, advanced radiation, and clinical trials exist at leading cancer centres in Mumbai, Delhi, Bangalore, Chennai, and Hyderabad. For most patients, travelling abroad is not necessary. What matters is finding a centre with a dedicated neuro-oncology team, high surgical volume, molecular testing capability, and access to trials — and those centres exist in India.
MGMT methylation status tells you how likely the tumour is to respond to temozolomide chemotherapy. Patients with MGMT-methylated tumours respond significantly better to temozolomide and have better overall outcomes than those with unmethylated tumours. It also influences decisions about treatment intensity, alternative chemotherapy agents, and trial eligibility. This is why MGMT testing should be done on every glioblastoma tumour before treatment begins — it directly shapes the treatment plan.
TTFields (Tumour Treating Fields) is an approved treatment for glioblastoma that delivers low-intensity, alternating electric fields to the scalp via a wearable device, disrupting tumour cell division. When added to maintenance temozolomide, it has been shown to extend median survival compared to chemotherapy alone. It is increasingly available in India — ask specifically whether your treating centre supports or offers TTFields as part of the treatment plan.
Yes — India has growing participation in international neuro-oncology clinical trials. Areas of active research include immunotherapy approaches (checkpoint inhibitors, tumour vaccines), targeted therapies based on molecular markers, novel drug delivery methods that overcome the blood-brain barrier, and combinations of existing treatments. Ask your neuro-oncologist explicitly what trials are currently open for your situation — both at diagnosis and at recurrence.