24 May 2026
Table of Contents
If you or someone you love has been diagnosed with relapsed or refractory lymphoma or hasn’t responded to standard therapy, you may have started hearing about CAR T cell therapy. And if you’re in Mumbai or anywhere in India, you may be wondering whether this treatment is accessible here or whether you’d need to travel abroad to access it. The answer is CAR T therapy for lymphoma is available in India. This guide walks you through everything you need to know.
CAR T therapy has fundamentally changed what’s possible for patients with certain relapsed lymphomas. For a meaningful proportion of patients who had exhausted standard treatment options, it has produced deep, durable remissions outcomes that simply weren’t achievable before. Understanding what it is, whether it applies to your specific lymphoma, and what the journey involves is the first step toward making the most informed decision for you or your loved one.
Understanding Lymphoma and When Standard Treatment Isn't Enough
Lymphoma is a cancer of the lymphatic system, a network of tissues and organs that form a key part of the immune system. It develops when lymphocytes (white blood cells) grow abnormally and accumulate in the lymph nodes, spleen, bone marrow or other organs. There are two main categories are Hodgkin lymphoma and Non-Hodgkin lymphoma, with Non-Hodgkin lymphoma being significantly more common and encompassing dozens of subtypes.
Most lymphomas respond well to initial treatment, typically a combination of chemotherapy with or without targeted therapy like rituximab. For many patients, this is sufficient. But for a significant proportion roughly 30-40% of patients with aggressive Non-Hodgkin lymphomas, the disease either relapses after achieving remission, or is refractory, meaning it never fully responded to first-line treatment. These patients are the ones for whom CAR T cell therapy has been most transformative.
Before CAR T, the standard approach for relapsed aggressive lymphoma was salvage chemotherapy followed by autologous stem cell transplant for patients who responded. For patients who didn’t respond to salvage therapy, or who relapsed after transplant, options were limited and outcomes were poor. CAR T has changed this picture significantly and it is now approved and available in India.
What Is CAR T Cell Therapy for Lymphoma?
CAR T cell therapy is a highly personalised immunotherapy, meaning it harnesses your own immune system, reprogrammed and redirected to find and destroy lymphoma cells. Here’s the clearest way to understand it: your immune system has T-cells whose job is to identify and eliminate threats. Lymphoma cells are very good at evading them, CAR T therapy gives those T-cells a new weapon, a specially engineered receptor called a Chimeric Antigen Receptor (CAR) that enables them to precisely recognise and attack lymphoma cells.
Because the treatment is built from your own cells, it is deeply personalised and because the CAR receptors are designed to target a specific marker on lymphoma cells, most commonly a protein called CD19, the attack is precise rather than the broad, body-wide impact of traditional chemotherapy.
Which Types of Lymphoma Can CAR T Therapy Treat?
CAR T cell therapy is currently approved and most established for B-cell Non-Hodgkin lymphomas, the group of lymphomas that arise from B-lymphocytes and carry the CD19 marker that current CAR T products target. Here’s where the evidence is strongest:
Diffuse Large B-Cell Lymphoma (DLBCL)
The most common aggressive lymphoma in adults. CAR T is approved for relapsed or refractory DLBCL after two or more prior lines of therapy and has produced durable remissions in patients with no other effective options
Primary Mediastinal B-Cell Lymphoma (PMBCL)
A subtype of large B-cell lymphoma arising in the chest. CAR T has shown strong activity in relapsed or refractory PMBCL and is now an approved option in this setting.
Follicular Lymphoma (FL)
A slower-growing lymphoma that often recurs over time. CAR T is now approved for relapsed or refractory follicular lymphoma after two or more prior therapies, a significant expansion of access for this patient group.
Transformed Follicular Lymphoma
When follicular lymphoma transforms into a more aggressive large B-cell lymphoma, CAR T therapy is an effective option for relapsed or refractory disease.
Mantle Cell Lymphoma (MCL)
An aggressive B-cell lymphoma that often becomes resistant to standard therapies. CAR T is an approved option for relapsed or refractory MCL, offering meaningful responses in a difficult-to-treat disease.
Research into CAR T for other lymphoma subtypes, including T-cell lymphomas and Hodgkin lymphoma is actively ongoing, with new targets and products in trials. If your specific subtype isn’t listed here, ask your haematologist whether any trials are relevant.
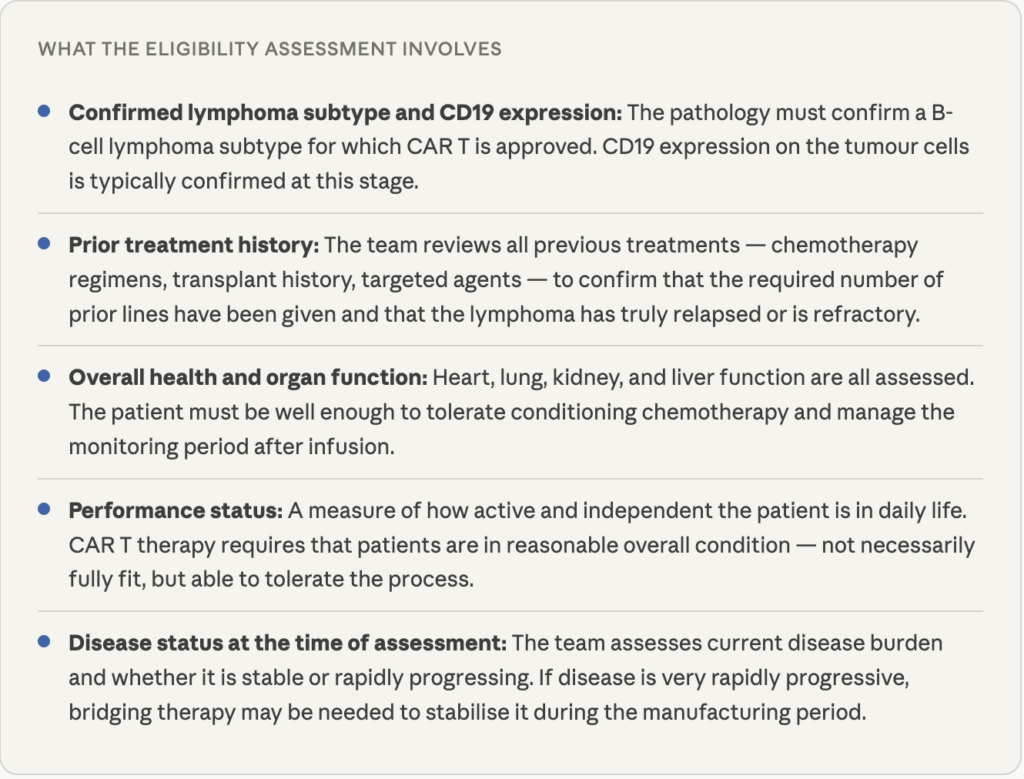
Who Is Eligible and What Does Eligibility Assessment Involve?
CAR T therapy is not suitable for every lymphoma patient, the eligibility is carefully and individually assessed. Generally, CAR T is considered when a patient has relapsed after two or more prior lines of treatment, or has refractory disease that hasn’t responded to standard therapy. Beyond diagnosis, several other factors are evaluated:
Being told you may not be eligible right now doesn’t mean never. Bridging therapy, a short course of treatment to stabilise the disease during the manufacturing period can sometimes make CAR T feasible for patients who aren’t immediately eligible. Ask your haematologist about this if eligibility is the current barrier.
The CAR T Treatment Journey: What to Expect Step by Step
The complete CAR T timeline for lymphoma patients
- Weeks 1-2 Eligibility assessment: Consultation, review of prior treatment history, blood tests, imaging, organ function tests, and confirmation of eligibility. This is also when the manufacturing slot is booked with the cell therapy facility.
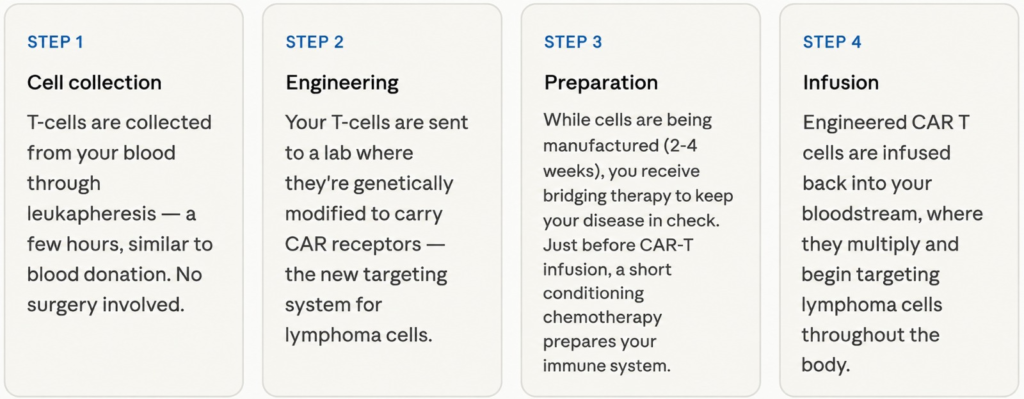
- Weeks 2-3 Cell collection (leukapheresis): T-cells are collected from the blood in a procedure taking a few hours, done on an inpatient or short-stay basis. Well-tolerated by most patients. Bridging therapy, if needed, begins around this time.
- Weeks 3-6 Manufacturing: The collected T-cells are sent to the cell therapy laboratory for genetic modification. This typically takes 2-4 weeks. The patient remains under the care of the haematology team during this period, often continuing bridging therapy.
- Week 6-7 Conditioning chemotherapy: A short, lower-intensity lymphodepleting chemotherapy course (typically fludarabine and cyclophosphamide) is given 2-7 days before infusion. This prepares the immune system to receive and support the CAR T cells. Hospitalisation required.
- Week 7 CAR T infusion: The engineered CAR T cells are infused, the infusion itself takes a few hours. Patients are admitted to hospital at this point for close monitoring by the experienced cellular therapy team.
- Weeks 7-9 Inpatient monitoring: The most critical period. The team monitors closely for cytokine release syndrome (CRS) and neurotoxicity (ICANS) the two main side effects and manages them promptly. Most patients are inpatient for approximately 2 weeks after infusion.
- Weeks 10 onward Outpatient follow-up: After discharge, regular outpatient visits, blood tests, and imaging continue for several months to assess response and monitor for late effects. The first response assessment, typically a PET-CT scan is done around 4 weeks after infusion.
The total journey from first consultation to discharge after infusion spans roughly 6-8 weeks. Staying within reasonable distance of the treating centre for at least 4-6 weeks after discharge is generally advised. For families travelling from other cities or states, the team will usually help you plan logistics, including what can be managed remotely and what requires in-person visits.
India has also seen the development of an indigenously manufactured CAR T product, making this treatment more accessible than it was even two years ago. If cost has been a consideration in your research, it is worth having a specific conversation with the treating team about the options available, including both internationally approved and Indian-manufactured products.
Frequently Asked Questions
Both are advanced treatments for relapsed lymphoma, but they work differently. In an autologous stem cell transplant, the patient's own stem cells are collected and reinfused after high-dose chemotherapy to reset the immune system. CAR T specifically engineers T-cells to target the lymphoma. For many relapsed lymphoma patients who have already had an autologous transplant or are not transplant candidates, CAR T is now the preferred next option with strong evidence of response even in patients who've failed transplant.
The two main side effects are cytokine release syndrome (CRS) a strong immune response causing fever, fatigue, and sometimes low blood pressure and ICANS (immune effector cell-associated neurotoxicity syndrome), which can cause temporary neurological symptoms like headaches or confusion. Both are anticipated, monitored closely from the time of infusion, and managed effectively at experienced CAR T centres. Most patients recover well with the right supportive care. This is one reason CAR T therapy must be delivered at a specialist centre with the right infrastructure and team experience.
The full process from first consultation to discharge after the monitoring period — typically spans 6-8 weeks. The manufacturing period alone (while your cells are being engineered) usually takes 2-4 weeks. After discharge, outpatient follow-up continues for several months. Staying within reasonable distance of the treating centre for at least 4-6 weeks after discharge is generally advised.
If lymphoma doesn't respond to CAR T or relapses after an initial response, further treatment options exist — including bispecific antibodies (such as mosunetuzumab or glofitamab), allogeneic stem cell transplant in selected cases, clinical trials of newer agents, and other salvage approaches. A non-response to CAR T doesn't mean all options are exhausted. Your haematologist at SUNACT will discuss what the next steps could look like based on your specific situation.