26 June 2026
Table of Contents
A Hodgkin lymphoma diagnosis can feel overwhelming, but here is something genuinely important to know at the outset: Hodgkin lymphoma is one of the most treatable cancers in medicine. With modern treatment, the majority of patients including those with advanced disease can be cured. That is not an overstatement. It is one of the great success stories of oncology, and it is as true in India today as anywhere in the world.
That said, “treatable” is not the same as “simple.” The decisions made about which treatment protocol to use, how to monitor response, and what to do if the disease persists or returns are consequential ones that require genuine haematological expertise. This guide will walk you through what modern Hodgkin lymphoma treatment in India looks like clearly, honestly, and with enough detail to help you ask the right questions and make the most informed decisions for yourself or your loved one.
What Is Hodgkin Lymphoma and How Is It Different?
Hodgkin lymphoma (HL) is a cancer of the lymphatic system, a network of tissues and organs that forms a key part of the immune system. It develops when B-lymphocytes (a type of white blood cell) undergo a specific malignant transformation, producing abnormal cells called Reed-Sternberg cells. These cells are the defining pathological feature of Hodgkin lymphoma and are what distinguish it from Non-Hodgkin lymphoma under the microscope.
What makes Hodgkin lymphoma clinically distinct from most other blood cancers is its behaviour as it tends to spread in an orderly, predictable pattern through the lymph node chains, rather than disseminating widely at an early stage. This makes it more amenable to treatment with chemotherapy and radiation, which is one of the primary reasons it has such high cure rates compared to other lymphomas.
Hodgkin lymphoma is most commonly diagnosed in two age peaks: young adults between 15 and 35, and adults over 55. It is slightly more common in men. In India, it accounts for a significant proportion of lymphoma diagnoses and importantly, it is diagnosed more frequently in younger patients in India than in Western countries, which means many patients are in their most productive years when diagnosed. This makes treatment decisions, particularly about long-term side effects especially important.
How Hodgkin Lymphoma Is Diagnosed and Staged in India
Hodgkin lymphoma most commonly presents as painless swelling of the lymph nodes, most often in the neck, armpits, or chest sometimes accompanied by systemic symptoms like persistent fever, night sweats, and unexplained weight loss (collectively called “B symptoms”). Itching and fatigue are also common.
Diagnosis requires a tissue biopsy, ideally an excisional biopsy of an accessible lymph node to confirm the presence of Reed-Sternberg cells and determine the subtype. Once confirmed, staging determines how extensive the disease is and directly guides treatment decisions.
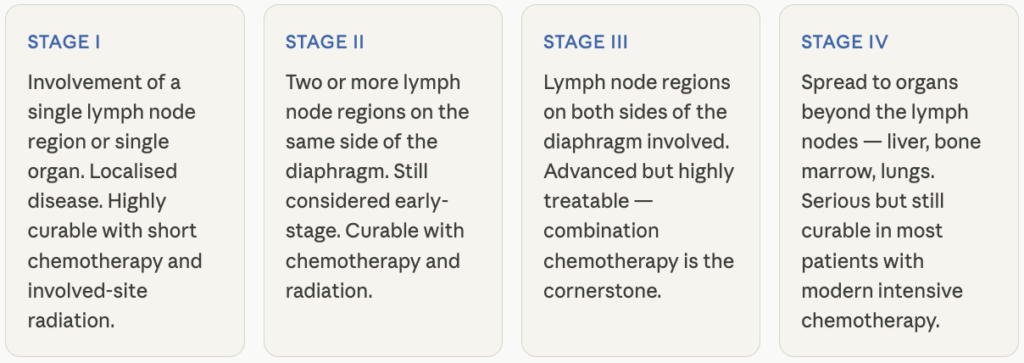
Staging is done using a PET-CT scan which is the gold standard for Hodgkin lymphoma which provides both anatomical and metabolic information about where disease is active in the body. PET-CT is central to both initial staging and response assessment during and after treatment, and should be standard at any centre managing Hodgkin lymphoma seriously. Bone marrow biopsy may be added in specific cases.
Modern Hodgkin Lymphoma Treatment Options in India
Treatment for Hodgkin lymphoma in India has kept pace with global advances, and the approach is tailored to each patient based on their stage and how well they respond along the way. Broadly, treatment involves three things: chemotherapy, radiation, and adjusting the plan based on how the body responds.
Chemotherapy
Chemotherapy is the foundation of Hodgkin lymphoma treatment for almost everyone. The standard regimen, called ABVD, combines four drugs given in cycles every two weeks, and it works well across all stages of the disease. For more advanced or higher-risk cases, doctors sometimes use a more intensive combination that can be more effective but also comes with more side effects, your haematologist will help weigh this trade-off based on your specific situation.
In recent years, a newer drug called brentuximab vedotin has also been added to frontline treatment for advanced-stage disease in some cases. It targets lymphoma cells more precisely and has helped improve outcomes while reducing certain side effects. It’s available in India and worth asking your doctor about if you have advanced-stage disease.
Radiation therapy
Radiation is often used alongside chemotherapy, particularly for early-stage disease or when there’s a localised area of concern. The good news is that radiation techniques have become much more precise over the years, treatment today targets a smaller, more specific area than it used to, which means fewer long-term side effects compared to older approaches. For more advanced disease, radiation is used more selectively, based on how the cancer has responded to chemotherapy.
Adjusting treatment based on response
One of the most important advances in Hodgkin lymphoma care is that doctors no longer follow a fixed plan from start to finish, they check in along the way. A PET-CT scan partway through chemotherapy shows how well the treatment is working. If the response is excellent, some patients can have less treatment than originally planned, fewer cycles of chemotherapy, or no radiation at all. If the response isn’t strong enough, the team may intensify treatment. This back-and-forth approach helps patients get exactly as much treatment as they need, not more, not less and it’s something to specifically ask your centre about.
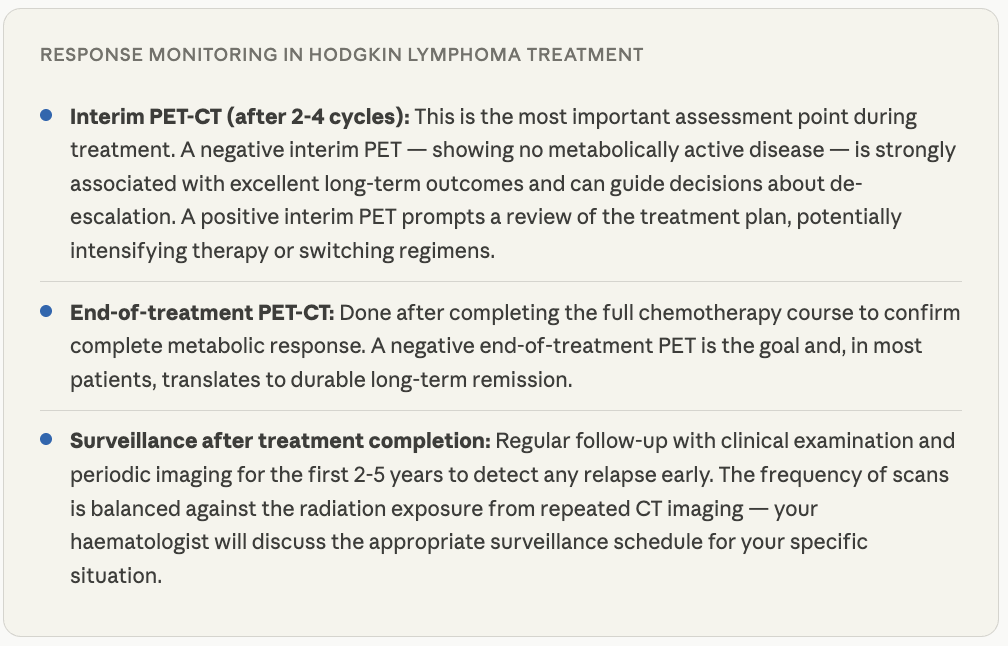
How Treatment Response Is Monitored
Monitoring response to treatment is fundamental in Hodgkin lymphoma, not just at the end of treatment, but during it. Here’s what that looks like in practice:
When Hodgkin Lymphoma Relapses: What Comes Next
Approximately 10-30% of Hodgkin lymphoma patients will relapse after initial treatment, or have refractory disease that doesn’t achieve remission. This is a challenging but important situation and crucially, it is one where further curative treatment is still possible for many patients.
Salvage chemotherapy and autologous stem cell transplant
The standard approach for relapsed Hodgkin lymphoma is salvage chemotherapy, using a different, platinum-based regimen to achieve a second remission, followed by high-dose chemotherapy and autologous stem cell transplant (ASCT) for patients who respond. ASCT consolidates the response and remains the standard curative approach for relapsed Hodgkin lymphoma. It is available at specialist bone marrow transplant centres across India.
Brentuximab vedotin
Brentuximab vedotin has established efficacy in relapsed or refractory Hodgkin lymphoma, both as a bridge to transplant and as maintenance therapy after transplant to reduce relapse risk. For patients who have relapsed after autologous transplant, brentuximab vedotin used alone has produced responses in a significant proportion of patients.
Immunotherapy- checkpoint inhibitors
Hodgkin lymphoma is one of the cancers most sensitive to PD-1 checkpoint inhibitors, drugs like nivolumab and pembrolizumab that release the immune system’s brakes. Response rates in relapsed or refractory Hodgkin lymphoma are among the highest seen with checkpoint inhibitors in any cancer, making these drugs an important option for patients who have failed transplant or are not transplant candidates.
Allogeneic stem cell transplant
For patients with multiple relapsed disease or who relapse after autologous transplant, allogeneic stem cell transplant using a matched donor’s cells offers the possibility of a graft-versus-lymphoma effect. It carries higher risks than autologous transplant but can achieve durable remission in selected patients at experienced BMT centres.
Life After Treatment: Long-Term Considerations
Because Hodgkin lymphoma is so frequently cured and diagnosed predominantly in young adults, the long-term effects of treatment are a critically important part of the conversation. This is one area where the expertise and thoughtfulness of the treating team makes a significant difference.
How to Find the Right Hodgkin Lymphoma Specialist in India
Hodgkin lymphoma is best managed by a haematologist or haemato-oncologist with specific experience in lymphoma, ideally within a centre that has a dedicated lymphoma programme. Here’s what to look for:
What to look for in a Hodgkin lymphoma treatment centre :
- Lymphoma-specific haematology expertise: Look for a haematologist who manages a significant volume of lymphoma cases of Hodgkin and Non-Hodgkin and stays current with evolving treatment protocols. The field moves quickly and expertise matters.
- PET-CT-guided response-adapted treatment: This should be standard practice. If a centre is not using interim PET-CT to guide treatment decisions, ask why. Response-adapted treatment is now established standard of care for Hodgkin lymphoma globally.
- Access to brentuximab vedotin and checkpoint inhibitors: For advanced or relapsed disease, access to these modern agents is important. Ask whether the centre offers brentuximab vedotin as part of frontline advanced-stage treatment and checkpoint inhibitors for relapsed disease.
- Stem cell transplant capability: For patients who relapse, autologous stem cell transplant is a core part of the salvage pathway. Ensure the centre has an established BMT programme or a clear referral pathway to one.
- Clinical trial access: For high-risk or relapsed disease, clinical trial participation can provide access to newer treatment combinations. Ask whether any trials are open for your specific situation.
Frequently Asked Questions
Yes, Hodgkin lymphoma is one of the most curable cancers, and that is as true in India as anywhere in the world. At experienced haematology centres in India, cure rates of 80-90% or higher are achievable for most stages of Hodgkin lymphoma. Even Stage III and IV disease has excellent cure rates with modern combination chemotherapy. The key is being treated at a centre with genuine lymphoma expertise and access to modern protocols including PET-guided response-adapted treatment.
Both are cancers of the lymphatic system, but they differ in the cell type involved, behaviour, treatment approach, and prognosis. Hodgkin lymphoma is defined by the presence of Reed-Sternberg cells and tends to spread in an orderly pattern, making it highly responsive to chemotherapy and radiation. Non-Hodgkin lymphoma encompasses many more subtypes with varying behaviour, from indolent to highly aggressive, and is treated with a much wider range of approaches. Hodgkin lymphoma generally has better cure rates than most Non-Hodgkin lymphoma subtypes.
For early-stage Hodgkin lymphoma, treatment typically involves 2-4 cycles of ABVD (or equivalent) followed by involved-site radiation, spanning roughly 4-6 months in total. For advanced-stage Hodgkin lymphoma, 6 cycles of chemotherapy (approximately 6 months) is standard, sometimes followed by radiation to initial sites of bulky disease. The exact timeline depends on the stage, regimen chosen, and response to treatment.
ABVD chemotherapy, the most commonly used regimen for Hodgkin lymphoma carries a relatively low risk of permanent infertility compared to more intensive regimens. However, fertility preservation (sperm banking for men, egg or embryo freezing for women) should be discussed before treatment begins wherever possible. More intensive regimens like escalated BEACOPP carry higher infertility risk, which is an important consideration in treatment planning for younger patients. Ask your haematologist about this explicitly before starting treatment.
Relapsed Hodgkin lymphoma is serious, but further curative treatment is possible for many patients. Salvage chemotherapy followed by autologous stem cell transplant is the standard approach and achieves durable remission in a significant proportion of patients. For those who relapse after transplant or are not transplant candidates, brentuximab vedotin and checkpoint inhibitors (nivolumab, pembrolizumab) have produced meaningful responses. Allogeneic transplant is an option for selected patients with multiply relapsed disease. If Hodgkin lymphoma relapses, prompt referral to a specialist lymphoma centre with BMT capability is essential.