14 March 2026
Table of Contents
Receiving a diagnosis of Multiple Myeloma can be an overwhelming experience. However, the landscape of haematological oncology in India has undergone a radical transformation. By combining world-class clinical expertise with significantly lower treatment costs compared to Western nations, India has emerged as a global hub for comprehensive myeloma care. This guide provides a detailed overview of the disease, diagnostic protocols, treatment pathways, and the practicalities of seeking specialised care in India.

What Is Multiple Myeloma? A Cancer of Plasma Cells
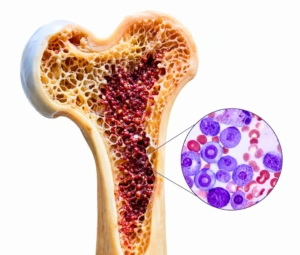
To understand Multiple Myeloma, one must first understand plasma cells. These are a specialised type of white blood cell found in the bone marrow, responsible for producing antibodies that fight infections. In Multiple Myeloma, these plasma cells become cancerous and multiply uncontrollably.
Instead of producing helpful antibodies, these malignant cells produce abnormal proteins called M-proteins. These proteins can cause extensive damage to the body, particularly the kidneys and bones. Because plasma cells reside in the bone marrow — the “factory” for all blood cells — their overgrowth crowds out healthy red cells, white cells, and platelets. This leads to common complications such as anaemia, increased susceptibility to infections, and brittle bones.
Diagnosis of Multiple Myeloma in India
Diagnosis usually begins when a patient presents with symptoms summarised by the medical acronym CRAB. Understanding these warning signs can lead to earlier intervention and better outcomes.
Calcium
Elevated levels of calcium in the blood caused by bone breakdown.
Renal
Kidney insufficiency or failure caused by the clogging effect of M-proteins.
Anaemia
Low red blood cell counts leading to persistent, unexplained fatigue.
Bone
Painful bone lesions or “punched-out” holes in the skull, spine, or pelvis.
Diagnostic Protocols Used in India
Indian specialists utilise a combination of advanced diagnostic tools to confirm the disease:
Bone Marrow Biopsy and Aspiration
To determine the percentage of cancerous plasma cells present in the marrow.
Protein Electrophoresis (Serum and Urine)
To detect the presence and level of M-proteins circulating in the body.
Free Light Chain (FLC) Assay
A sensitive blood test used to monitor disease progression over time.
Advanced Imaging: Whole-Body MRI or PET-CT
Now standard in Indian hospitals to identify bone damage that traditional X-rays might miss.
Staging: The Revised International Staging System (R-ISS)
Most Indian oncologists use the Revised International Staging System (R-ISS). This categorises the disease into three stages based on blood markers, chromosomal abnormalities (cytogenetics), and LDH levels. Accurate staging is vital as it dictates whether a patient requires aggressive “quadruplet” therapy or a more standard approach.
Stage I
Low-risk features. Standard regimens are typically sufficient for effective disease control.
Stage II
Intermediate risk. Treatment is personalised based on individual blood markers and cytogenetics.
Stage III
High-risk features present. Aggressive quadruplet therapy is usually recommended at experienced centres.
Why Staging Matters
Staging directly determines the intensity of treatment — under- or over-treating carries its own risks.
Multiple Myeloma Treatment Options in India
Treatment for Multiple Myeloma in India is highly personalised, moving away from generic chemotherapy towards targeted regimens. The treatment journey typically follows a structured pathway.
Phase 1
The first phase aims to reduce the cancer burden. Modern Indian protocols often use a triplet or quadruplet regimen. This typically includes a combination drawn from the four drug classes below.
Phase 2 — Gold Standard
For patients who are physically fit, ASCT remains the gold standard. The patient’s own healthy stem cells are collected, high-dose chemotherapy is administered to clear the marrow, and the stored cells are re-infused to “reboot” the system. It is a medical process, not a surgical one.
Phase 3 — The Frontier
CAR-T products for Multiple Myeloma (targeting the BCMA protein) are currently available primarily through advanced clinical trials and compassionate use programmes at premier institutes. Bispecific T-cell Engagers (BiTEs) are increasingly being used in relapsed cases at leading private centres.
Drug Classes Used in Induction Therapy
Proteasome Inhibitors
e.g., Bortezomib, Carfilzomib — block the cellular “waste disposal” system, causing cancer cells to self-destruct.
Immunomodulatory Drugs (IMiDs)
e.g., Lenalidomide — stimulate the immune system to recognise and attack myeloma cells.
Monoclonal Antibodies
e.g., Daratumumab — target a specific protein (CD38) found in high quantities on myeloma cells.
Steroids
e.g., Dexamethasone — used alongside other agents to enhance effectiveness and manage inflammation.
India’s CAR-T Cell Progress
While India has successfully launched indigenous CAR-T cell therapies for Lymphoma (NexCAR19), CAR-T for Multiple Myeloma is currently in the clinical trial phase. It is expected to become commercially available in the near future — making India one of the few countries developing home-grown cellular therapies for this disease.
How to Choose the Right Hospital and Specialist in India
A Bone Marrow Transplant (BMT) involves a period where the immune system is essentially “switched off.” Therefore, the choice of hospital is as critical as the procedure itself. When evaluating Multiple Myeloma treatment centres in India, look for these essentials:
Infection-Control Infrastructure
The unit must have HEPA-filtered rooms with positive pressure to prevent airborne fungal and bacterial infections while the patient’s immune system is suppressed.
MDT Expertise
Prioritise centres with a dedicated Haemato-Oncology Multidisciplinary Team (MDT) that includes infectious disease specialists and specialised nutritionists.
Comprehensive Cellular Programmes
Choose a centre that offers both BMT and CAR T-cell therapy (or clinical trials for it). This ensures they can manage complex relapses without needing to transfer your care elsewhere.
24/7 Support and Cost Transparency
Ensure the centre provides around-the-clock clinical access post-discharge and a full, itemised cost estimate that includes preparatory chemotherapy, infection-prevention drugs, and long-term follow-up.
What Outcomes Should You Expect?
Multiple Myeloma is no longer the “death sentence” it was once considered. With access to modern targeted therapies at experienced Indian centres, the expected outcomes are encouraging.
80–90%
Approximately 80–90% of patients achieve a significant reduction in cancer markers after initial therapy.
8–10+
With access to modern drugs, many patients now live 8 to 10 years or longer, maintaining excellent quality of life.
MRD–
The new treatment goal — reaching MRD negativity — means no cancer cells detectable even at a molecular level.
Frequently Asked Questions
“Multiple Myeloma is no longer the ‘death sentence’ it was once thought to be. With India’s unique blend of medical expertise and cost-effective innovation, patients have more reasons for hope than ever before.”