13 March 2026
Everything you need to know about HSCT for your child — explained clearly, step by step.
Table of Contents
If your doctor has mentioned Hematopoietic stem cell transplant for your child, you’re probably feeling worried, confused, maybe even fearful. That’s completely normal. This guide is here to walk you through what stem cell transplant really means, when it’s needed, and what you can actually expect.
What Exactly is a Hematopoietic Stem Cell Transplant?
Think of stem cells as your child’s body’s master builders. They’re special cells that can turn into any type of blood cell your child needs, red blood cells that carry oxygen, white blood cells that fight infections, and platelets that help blood clot.
When do doctors recommend this for kids?
Hematopoietic stem cell transplant treats several serious conditions:
- Blood cancers like leukaemia and lymphoma
- Blood disorders including thalassaemia major, sickle cell disease, and aplastic anaemia
- Immune system problems like severe combined immunodeficiency (SCID)
The goal? To cure the disease or give your child a normally functioning blood and immune system.
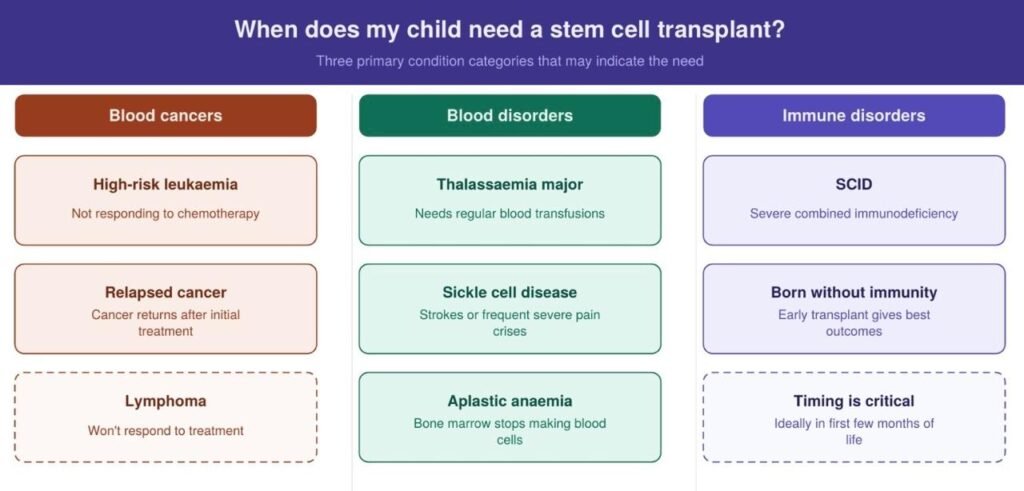
So When Does My Child Actually Need This?
Bone marrow transplants can be life-changing for children with certain blood cancers, blood disorders, and immune conditions. The decision to proceed depends on how serious the condition is, how well other treatments are working, and whether a suitable donor match can be found. Let’s look at when doctors typically recommend this treatment for different situations.
What's the Actual Process Like?
Step 1: Getting Ready (2-4 Weeks)
Your child will go through lots of tests, blood work, scans, heart and lung checks. This makes sure they’re strong enough for the treatment.
Meanwhile, the team starts looking for a donor. Siblings get tested first since they have a 1 in 4 chance of being a perfect match. And if the sibling doesn’t match? They’ll search national and international donor registries.
Your child will also get a central line which is a special IV that stays in place. It sounds scary, but it means way fewer needles during treatment.
Step 2: Conditioning (5-10 Days)
In this part your child gets high-dose chemotherapy (and sometimes radiation) to wipe out their diseased bone marrow and make room for the new stem cells.
Side effects can be nausea, mouth sores, fatigue, hair loss. But the medical team has ways to help manage these symptoms and keep your child as comfortable as possible.
Step 3: Transplant Day
The actual transplant looks just like a blood transfusion where stem cells flow through the central line over a few hours. It’s painless.
Those stem cells will travel through the bloodstream and find their way to the bone marrow, where they’ll settle in and start growing.
Step 4: The Waiting (2-4 Weeks)
At this time your child basically has no immune system, so they’ll be in isolation to protect them from infections. The team watches blood counts daily, waiting for signs that the new stem cells are working. Usually within 2-4 weeks, you’ll start seeing rising white blood cell counts.
Step 5: Recovery in Hospital (4-8 Weeks Total)
Even after engraftment happens, your child stays in the hospital for monitoring. They’ll get antibiotics, nutritional support, blood transfusions as needed, and medications to prevent complications.
As their blood counts improve, they’ll start eating better, more energy, and feel stronger each day.
Step 6: Going Home
Your child can go home when their blood counts are stable, there’s no infection, and they can take medications by mouth.
But you’ll need to stay near the hospital (within 30-60 minutes) for at least the first 100 days. Clinic visits will be frequent sometimes 2-3 times a week at first.
Most kids can return to school within 3-6 months, though with some restrictions at first.
What Are the Success Rates in India?
Good news India’s top paediatric transplant centres are achieving results that match international standards.
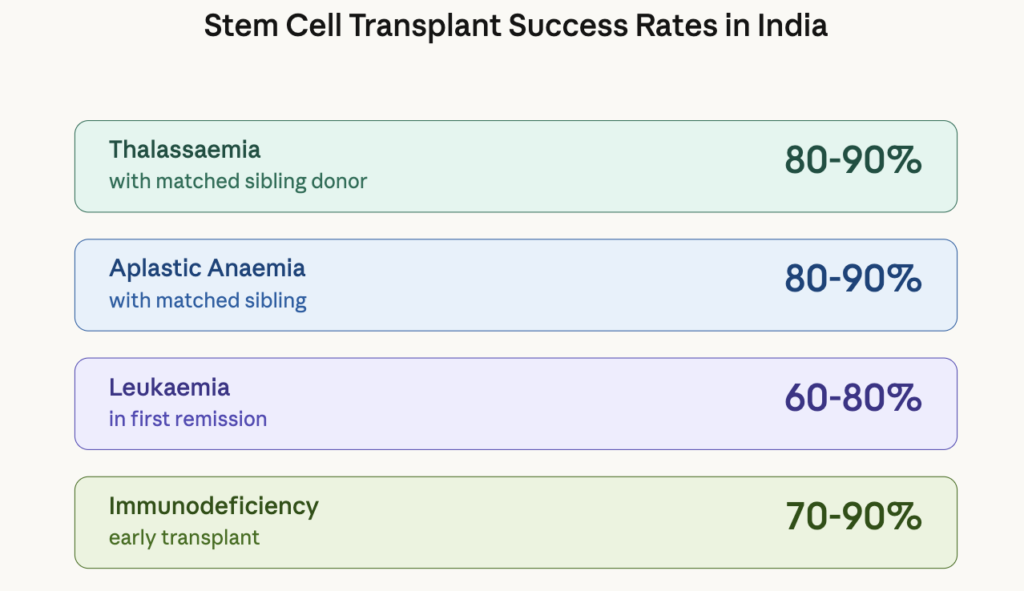
What affects these numbers?
Several things influence your child’s specific odds: how well the donor matches, whether the disease is in remission, your child’s age and overall health, and the experience of the transplant centre.
Frequently Asked Questions
Absolutely. Siblings are often the best donors. Each of your children has a 25% chance of being a perfect match with their brother or sister. If a sibling matches, they can donate through a bone marrow collection (under anaesthesia) or peripheral blood collection (similar to blood donation). It's very safe for healthy kids and bone marrow regenerates completely in 4-6 weeks. No perfect sibling match? Sometimes parents or half-matched siblings can donate using newer techniques that have gotten much better in recent years.
Plan for 4-8 weeks in the hospital, though every child is different. Here's the typical breakdown:
- Pre-transplant prep: 3-7 days
- Conditioning treatment: 5-10 days
- Transplant day: 1 day
- Waiting for engraftment: 2-3 weeks
- Post-transplant monitoring: 1-2 weeks
If complications happen like infections, severe graft-versus-host disease, the stay could stretch to several months. After discharge, plan to stay near the hospital for at least 3-4 months total.
Short-term concerns:
- Infections are the biggest worry since your child has basically no immune system for weeks
- Bleeding from low platelet counts
- Graft-versus-host disease where donor cells attack your child's body
- Mouth sores that make eating painful
- Organ stress from high-dose chemo
Long-term concerns:
- Chronic graft-versus-host disease affecting skin, eyes, liver
- Growth delays or hormone issues
- Possible fertility problems down the road
- Small increased risk of secondary cancers years later
- Learning or attention difficulties in some kids
Here’s the perspective to keep: Modern transplant techniques and experienced teams have made transplants much safer than they used to be. Your doctors will discuss your child’s specific risks and how they plan to minimize them.